Truncus arteriosus in India
Truncus arteriosus is a rare congenital heart defect that will need an open-heart surgery to repair
What is Truncus arteriosus?
Truncus arteriosus (TA) is a rare congenital heart defect. It is a major heart defect that causes affected babies to breathe faster, drink milk with difficulty, and be prone to catch lung infections.
In a normal healthy heart, you will have two major blood vessels coming out of the heart. In babies with this defect, the structure of the heart is altered. So, there is just one blood vessel that does the work of two vessels in a healthy heart. There is also a hole in the heart.
Truncus arteriosus will need open-heart surgery to repair. It is ideal to do the surgery before the baby is a month old. Undue delay can lead to severe complications.
What causes Truncus Arteriosus?
TA is a developmental disorder present at birth. What exactly causes it is not very clear. There are certain factors affecting mothers during pregnancy that increase the risk of TA and other heart defects in babies.
Some of the known risk factors are a family history of heart defects, mother on certain medications in early pregnancy, diabetes in mother from early pregnancy, IVF pregnancy, anomaly scan showing a defect in any other organ system of the fetus (brain, gut, kidney, etc.), mother indulging in alcohol/smoking in early pregnancy, German measles, high fever in early pregnancy.
Since the formation of the heart happens in the first two months of pregnancy, it is then that the above factors play a role! Apart from these, babies with chromosomal disorders like DiGeorge syndrome and velocardiofacial syndrome are more at risk. Truncus arteriosus can also occur in babies without any of these risk factors.
How blood flows in a heart with Truncus Arteriosus
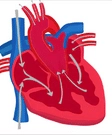
It is important to know how the normal heart works to understand TA better. See figure 1 below.

The left and right parts of the heart have two chambers each. The top two, the right artery(RA) and left artery (LA), are the collecting chambers. The bottom two are the pumping chambers, which are the right ventricle(RV) and left ventricle(LV).
The LV pumps the blood from the heart to the whole body through the aorta. The body's organs use the oxygen in that blood and make the blood impure.
This impure blood then returns to the RA. The RV pumps this to the lungs through the pulmonary artery.
When we breathe, the oxygen in our breath enters the blood and makes it pure again. The purified blood enters LA and is pumped out to the body by the LV.
Thus the heart supports two circuits. The left circuit pumps pure blood to the body, and the right circuit pumps impure blood to the lungs.
In a child with a TA, there are no separate aorta or pulmonary artery. Instead, blood exits the LV and the RV through a vessel (called Truncus). It continues as both the pulmonary artery and the aorta.
There is a large hole in the wall (septum) between the LV and the RV. So, blood flows from the LV and RV to the TRUNCUS. It then flows to the lungs and from there to the body. Every part of the body receives a mixture of pure and impure blood. It also means extra blood ends up going to the lungs. The congested lungs get infected relatively easily. The heart becomes bigger, and pressure on the right side of the heart also rises over time.
Symptoms of Truncus Arteriosus
Some of the common signs and symptoms of babies with TA include
- Breathing problems- Babies will exert while breathing. The breathing will be fast and shallow as well.
- Poor feeding- Babies tend to drink less than normal as they get tired during feeding (suck-rest-suck cycle).
- Excessive sleepiness
- Pounding of heart and an increase in heart rate.
- Bluish discoloration of the skin
Usually, the baby fails to thrive and shows poor growth if it does not get proper treatment at the earliest.
Complications of Truncus Arteriosus
A delay in treatment can cause severe complications. Some of the common ones are
- Severe breathing difficulty due to the collection of fluid in the lungs
- Pulmonary hypertension, where the blood pressure in the lungs stays high for months or more.
- Enlargement of the heart
- Heart failure due to worsening of complications
Diagnosis of Truncus Arteriosus
The doctor will do a few tests if your baby shows any signs and symptoms of Truncus arteriosus.
- Echocardiogram- This is the most important test for diagnosis. It is the ultrasound of the heart. It details the structure of the heart and gives the doctor team a good idea of how to proceed further.
- Chest X-ray- It will show the lungs' condition and the presence of fluids in the lungs.
- CT scan: In some cases, the Echocardiogram will not clearly show the branches of the pulmonary arteries. In such cases, the doctor may ask for a CT scan.
- FISH test: this blood test is to detect chromosome abnormalities in the baby (DiGeorge Syndrome). The FISH stands for Florescent InSitu Hybridization. If the baby has this, then the doctor team has to pay special attention to avoiding infections in the baby. It is crucial to keep track of his/her blood calcium levels.
The baby may also need a longer stay in the ICU after surgery. After discharge home, your baby with DiGeorge syndrome may have developmental delay and may need daily calcium supplements and extra vaccines for preventing infections.
Types of Truncus Arteriosus:
There are different types of TA based on the anatomy of the Truncus. The types of TA have implications for the surgical team. A certain type (associated with narrowing of the aorta) may need surgery sooner than other types.
Truncus arteriosus surgery - When to do?
If your baby has truncus arteriosus, he or she will need surgery to repair it at the earliest. It is best to do the surgery at a month of age, certainly before 3months of age. After 3months of age, the risk is higher.
Surgery for truncus arteriosus
The surgery team will have
- Neonatal heart surgeon
- Pediatric cardiologists
- Anesthetists
- Intensivists
- Nurses and supporting staff
Your baby will have an open-heart surgery under general anesthesia.
Before surgery
The surgeon will explain what happens during surgery and what to expect in the ICU later. They will tell you about the possible risks and complications as well. Once you give your consent, the surgical team will start preparations for the surgery at the earliest.
Your baby will have a few medicines before surgery. These medicines help to make operation easier and also to keep the baby stable during surgery.
During surgery
During the surgery, the surgeon will perform a few complex tasks. The first step is to separate the Pulmonary Artery from the aorta carefully. The surgeon will then connect this branch to the RV with the help of a tube or conduit. Then the hole in the heart is closed. The duration of the operation will be about four to five hours.
After surgery
Soon after surgery, the surgical team will move your baby to a pediatric cardiac intensive care unit. The doctor/nursing staff will continuously monitor the progress of your baby.
Your baby will have a few tubes and wires coming out from the body. All these are to help your baby to recover. Your baby will also have assistance with breathing through a breathing machine (ventilator) for a few days. Your baby will have food through a tube running from his nose (or mouth) to the stomach.
Once your baby starts recovering well, the tubes and wires will disappear one by one. By the end of the first week, your baby will come back to the room. You remain in the hospital for a few days more. Complete recovery will take a few weeks.
Aftercare
Your baby will not have any major restrictions after surgery. He or she will grow like a normal child.
But like any other heart defect by birth, your baby will need periodic heart check-ups.
As your baby grows, the tube's size may not be sufficient to allow enough blood to pass through it. In such situations, your baby will need surgery to replace the tube with a larger one. Life continues as normal, after replacement.
Top Hospitals for Truncus arteriosus
We partner with India's most respected accredited hospitals.






Frequently Asked Questions
Truncus arteriosus is a rare type of congenital heart defect. In a normal heart, there are 2 blood vessels, the pulmonary artery and aorta, coming out from the right and left ventricles. These two blood vessels start off as one in the mother’s womb and splits into two as the heart develops. In some babies, it does not split and so there is only blood vessel, which is the truncus arteriosus
Yes, truncus arteriosus can be cured with surgery. Babies will need surgery within the first few weeks after birth. In most cases, they will need follow-up surgeries as they grow up
Yes, it can be life threatening if not treated in time. Infants will not survive the first few months without treatment. The right time for the surgery is in the first month after birth
Surgery is the best option to fix truncus arteriosus. The surgeon will first close the VSD, which is a hole between the right and left ventricles. Then, the surgeon will separate the branch that goes to the lungs from the truncus arteriosus and connect it to the lungs. This becomes the pulmonary artery. Next step is to reconstruct the aorta from the truncus arteriosus and connect it to the left ventricle
Get a Free Quote
We respond within 2 working hours.
Request Received!
A coordinator will contact you within 2 working hours.